Every third urban resident over 55 years has some signs of joint diseases. Often, a pain in the hip joint and limited mobility is considered as the age norm, and people do not worry about it. Only when the pain becomes intense and prolonged and causes the gait changes, it becomes clear that it is a time to see a doctor.
With any diseases of the hip joint, whether it is arthritis or arthrosis, there is a certain risk of disability. Of course, if the treatment is started timely and a patient is under constant supervision of experienced doctors, there is a good chance to keep the mobility of the joint long enough.
But it also happens that conservative treatment is unsuccessful, the patient gradually loses the ability to move normally, and hip endoprosthesis surgery seems the only reasonable option.
Arthrosis and osteoporosis are constant companions of elderly people, with women suffering from functional pathologies 2 times oftener than men. In the main, the both diseases are associated with age hormonal changes in the body and decrease in the synthesis of bone cells. With osteoporosis, the bones become brittle, whilst with arthrosis, joint cartilage thins out. Both these forms of joint dysfunction are not inflammatory.
The supply of a hip endoprosthesis is the most common supply of an artificial joint on the human body. It is currently performed around 220,000 times a year in Germany. The principle consists in an artificial replacement of the acetabular cup and the femoral head after the conservative, i.e. non-operative therapy has been exhausted. This is possible with different types and materials of prosthesis.
The chances of success of the artificial hip joint are high. A high level of satisfaction can be expected in around 95 percent of all cases. Regardless of this, this is a surgical intervention that should be discussed extensively between doctor and patient in each individual case. Because like any other surgical procedure, the hip endoprosthesis naturally has potential risks and complications. With a good indication (that is, the intervention is appropriate in the patient's individual disease situation) and an experienced surgeon, hip arthroplasty can be viewed as a low-complication procedure.
Diagnostics
Destructive processes develop slowly, revealing themselves occasionally in attacks of sharp pain or difficulties to make usual movements, such as squatting, lifting, or turning. Gradually, the cartilage loses its elasticity and becomes thinner and thinner. Finally, the joint bones start rubbing against each other when walking, which leads to rapid deterioration of the joint surfaces. Excess weight, overloading the musculoskeletal system, makes the situation even worse.
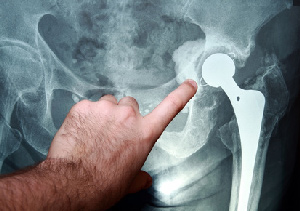
An orthopedist can determine the degree of arthrosis or osteoporosis by the patient’s gait, but the final conclusions can be made only based on an X-ray or MRI scan. If conservative treatment cannot help to restore the joint ligament function, scheduled hip replacement is considered, as further development of the disease may lead to disability. Emergent hip replacement for elderly is often done in case of the femoral neck fracture.
The X-Ray or MRI scan clearly shows the degree of degenerative changes in the bones and articular cartilage, as well as types of deformities and other abnormalities that can be eliminated with surgery by replacing a damaged part of the joint with a prosthesis.
If your surgeon has concluded the surgery as the only effective method of treatment for joint degeneration, it is not that sad, as you may think first.
If the components of the joint are severely damaged, radical surgery is not recommended. Fragile bones and atrophied ligaments may not be strong enough to hold an endoprosthesis, which leads to further deterioration of the joint and can cause a trauma. Therefore, if your doctor finds the hip joint surgery possible and beneficial, it can be considered good news.
Contraindications to Hip Arthroplasty
There are a number of diagnoses that are absolute contraindications to joint surgery:
- Chronic diseases in the stage of decompensation, including heart failure, ventricular and atrial arrhythmias, stroke complicated by neurological disorders, and impaired liver or kidney function;
- Diseases of the respiratory system (particularly, the lungs), accompanied by pulmonary ventilation disorders, such as bronchial asthma, pneumosclerosis, and bronchiectasis;
- Inflammation of the skin, muscles or bones in the area of the hip joint;
- Paresis or paralysis of the limb;
- Osteoporosis of the third or fourth degree (in this case, surgery is inexpedient, since a repeated fracture can occur even when simply walking);
- Hematopoiesis disorders;
- Severe mental disorders;
- Glaucoma;
- Childhood age (when musculoskeletal system in the stage of development).
Relative contraindications to joint replacement surgery are functional chronic diseases in the stage of remission, neurosis, diabetes mellitus, bone and joint deformities, inclination to allergic reactions, and excess weight.
What Is an Endoprosthesis?
You should take your time when choosing an artificial hip joint, or endoprosthesis, as your quality of life after surgery depends on the properties of this medical device. But you have also another option: to choose the right clinic you can trust. Taking into account that German surgeons do not use materials of poor quality, you can minimize your risks. If you add to this high skill and experience of the doctors underlying their professional success, you will see why services of German orthopedists are in demand.
During the preparation for the surgery, a doctor will tell you which hip prosthesis can be used in every particular case and will explain the advantages and possible disadvantages of different designs. You will get comprehensive information about artificial joints used in the clinic and advice of an expert, which can help you to make a well-thought-out decision.
Modern hip endoprostheses are complex devices. “Eternal” artificial hip joint has not been invented yet, but today there are some high-end models on the market with lifetime 15-20 years or even more. There are also cheaper analogues, with lifetime about 5-10 years. An artificial hip joint with cementless fixation consists of a ball (head), a stem, a cup and, also, an insert. Endoprosthesis with cement fixation consists of the same elements, but acetabular component is solid and not divided into the cup and insert. Each of the elements has its own size range. During replacement surgery, a surgeon selects and inserts the appropriate size individually for every patient.
There are a few types of fixations of the artificial hip joint:
- Cementless fixation;
- Cemented fixation;
- Hybrid fixation.
Depending on whether all the joint parts are replaced or not, there are total hip implants and partial hip implants.
The bearing is what provides rotation and movement in the artificial joint. The lifetime of the endoprosthesis depends on the type and quality of bearing materials.
Hip joint implants can be split into the following categories based on the bearing materials:
- Metal-on-metal (MOM)
- Metal-on-polyethylene (MOP)
- Ceramic-on-ceramic (COC)
- Ceramics-on-polyethylene (COP)
Same as with people’s faces, all of which different, there are no two identical joints in nature. Each person has specific anatomical features of the skeletal system, such as differences in size, shape and proportions of muscles, tendons and ligaments. That is why a number of sizes of implants are produced: a variety of models allows you to choose the option appropriate just for you. The ideal fitting of the implant stem and the joint is achieved by the femoral canal preparation.
A stem for cementless fixation has a rough surface, which allows the bone tissue to ingrow into the prosthesis. This type of prostheses is called a “press-fit” implant, which means the stem is simply inserted into the femoral canal after the preparation purposed to make it fitting to the prosthesis.
For cementless joint implants, titanium-based alloys with the best biocompatibility are used. The stem of the prosthesis is covered with calcium hydroxyapatite or another porous compound to accelerate the process of bone ingrowth into the artificial material.
All implant manufacturers have their own specifications to feature the prosthesis to the specific purposes. For better fitting in the bone canal, the stem can be finished with protruding elements, as pins and wings, and others. Selection of the stems is based on an X-rays scan. An orthopedist fits prepared femoral stem necks in order to choose the best one, meeting the femur morphology.
The stems may have cylindrical, conical or curved shape. As well as, their cross sections may be round or quadrangular. Whatever the implant design, it should meet the main task which is to ensure uniform distribution of load to the bone, along the length of the femoral canal and circumferentially.
A cup (socket) of the hip implant is a part of the prosthesis fixed in the acetabulum by a cement or cementless method. Acetabular component can be hemispherical or low profile (with a smaller bulge).
Low profile designs provide a wider range of movements, but, at the same time, they are less reliable at high loads, since low rims cannot prevent the dislocation of the femoral head from the endoprosthesis socket. In recent years, modernized designs have become widespread, in which the sides of the cup are strengthened.
The cement fixation cups are made of high molecular weight polyethylene; cementless sockets are made of an alloy of titanium with aluminum and niobium. The surface of the cementless cups is rough with a porous coating. There are also holes for fixing rods on the surface of the socket of hip implant.
Types of Hip Arthroplasty
Hip joint arthroplasty is an operation to replace a part of the joint with an artificial component (an implant). A variety of surgeries in this area can be divided into two groups: partial and total joint replacement. Hip hemiarthroplasty (partial replacement) is the replacement of the femoral head, while the acetabulum is kept. With total arthroplasty, both the acetabulum and femoral head are replaced.
The type of surgery treatment is decided by an orthopedic surgeon with consideration the following factors:
- Patient’s age
- Condition of bones and cartilage
- Kind and origin of joint deterioration (trauma or disease)
- General health of the patient
Older patients are more likely to have partial arthroplasty, since this type surgery is more sparing, and is not associated with excessive blood loss. But it has such disadvantage as a relatively short life of the endoprosthesis (5-6 years).
Total hip arthroplasty is a complex surgery. First, cartilage and subchondral bone tissue are removed and the joint surfaces are sawed, after which an implant is installed applying cement or cementless fixation. There are some disadvantages:
- the patient is under general anesthesia for a long time
- soft tissue damage
- significant blood loss
The main advantages are a long life of the implant and complete restoration of the joint functioning.
The method and surgical approach to the joint are selected during the preparation, taking into account several factors:
- Nature and extent of pathology;
- Condition of osteoarticular tissue;
- Health and age of the patient;
- Experience and skill of the surgeon.
The surgical technique depends much on the chosen approach to the joint. The incision can be anterior, anterolateral, posterior, and combined.
Posterior approach – which is the most physiological and causes minimal damage to the soft tissues, nerves and muscles – is the most common for hip arthroplasty. It also reduces the probable damage to the outflow mechanism.
For secondary surgeries that are required in case of surgeon’s mistake, implant rejection or repeated trauma, longer incisions are normally used. Open access provides a better view of the femur. It can be a longitudinal straight incision, or curved cut.
After the incision is made, the surgeon gently pushes the muscles and fascia aside, opens the joint capsule, and performs a resection of the damaged fragments. Then, the femoral head is removed and the acetabulum is thoroughly cleaned (With the total arthroplasty, the acetabulum is removed together with the femoral head).
The next step is the femoral component fixation with metal rods or cement, and, then, testing the distal area of the artificial joint. If there are no any deviations, the surgeon treats the medullary canal where the implant stem is inserted, and the implant head is attached to the acetabulum (an artificial hemispherical cup). After the total or partial prosthesis is placed, the wound is sutured layer by layer, and drainage is inserted.
Cap prosthesis (McMinn hip)
The "Birmingham Re-surfacing Hip" developed by the English surgeon Derek McMinn consists of a cap with which the femoral head is crowned like a tooth. The cap has only one pin for anchoring, so that the medullary canal of the thigh does not have to be opened. In addition, the large diameter of the hip prosthesis ensures extensive luxation security. Even today, the bone-saving prosthesis with the right indication is still considered an ideal alternative for the treatment of younger, normal-weight patients without femoral neck deformity.
Short shaft prosthesis
Short stem prostheses are today considered to be as stable as classic long stem prostheses, but due to the shorter overall length, they can be better implanted through minimally invasive approaches. Thus, bone and soft tissue is saved, which facilitates subsequent revision surgery and favors a quick healing after hip surgery. In the medium term, experts see the short shaft prosthesis as the first choice, especially for the care of physically active patients with good bone quality.
Normal stem prosthesis
The standard stem prosthesis is the gold standard of hip prosthetics. The lifetime of modern implants is considered to be very good, but relatively much bone is sacrificed during implantation. However, due to its universally good properties, it is especially the first choice for older patients who can expect this
Hip prosthesis to be optimally cared for life.
Complications After Surgery
Complications after hip arthroplasty are rare, but you should be aware of the possible consequences, among which the most likely are:
- Wound Infection
- Blood clots
- Implant rejection
- Implant Dislocation
- Exacerbation of chronic diseases
After hip surgery, the patient is under constant monitoring by a medical team, so the risks of adverse effects are minimized. Today, surgery and recovery are performed according to the detailed step-by-step procedures, which reduces the likelihood of unforeseen situations.
Revision Endoprosthetics
Revision hip surgery is a secondary operation that is used in case of serious complications after implant placement, including:
- Aseptic loosening of the joint components;
- Purulent infection;
- Fracture of the implant stem;
- Scarring in the area of the joint cup.
Hip joint revision techniques are fundamentally different from those applied in the primary surgery. Hip joint replacement is carried out according to standardized protocols, but revision method is decided individually every time and every surgery is unique.
A complicating factor is a significant loss of bone tissue surrounding the endoprosthesis. The surgeon must remove the cement joint, clean the articular surfaces, and, then, install new implant components.
With the development of total purulent process, it is not always possible to perform joint restoration with an implant, since sepsis spreads quickly to soft tissues and organs. Fortunately, purulent infection is an extremely rare complication after surgery. Basically, revision is possible to eliminate all defects appeared after primary surgery.
Surgery Satisfaction
According to statistics, hip joint replacement surgery mostly has positive reviews. Patients are satisfied with the results. When performing surgery in relatively young age and without concomitant diseases, functioning of the hip joint can be fully restored. You can walk and even exercise, avoiding overloading the artificial joint. Active sports are contraindicated. There are also some unsatisfactory results after hip arthroplasty. Most often they happen in old age, if there are any concomitant pathologies. The patients' feedbacks show disappointment with the surgery results in 20% of patients who had hip joint replacement.
About Implants for Hip Endoprosthesis
BIOLOX®. Patient information on hip joint implants
CeramTec stands for high-quality ceramic hip joint replacement. High-performance ceramics that set standards. For more than 40 years, we have been at the forefront of research, development and production in the field of bioceramics worldwide. Over 10 million patients on all continents testify to the medical success of our products.
Worldwide, surgeons rely on pink BIOLOX®delta ceramics.
Even the color gives the surgeon the certainty of using hip implants of the highest quality and safety for his patients from CeramTec.
BIOLOX®delta is the only ceramic with 15 years of successful clinical experience and more than 8 million sold components.
Materials for hip joint implants
Different components made of different materials.
Today's endoprostheses consist of various components of modular hip joint systems.
There are the following pairings:
- Metal / polyethylene
- Ceramic / polyethylene
- Pottery / Ceramics
- Metal / Metal
The pan housing (metal shell) used in the pelvic bone is equipped with a pan insert. The socket insert represents a joint surface of the endoprosthesis. The ball head, which is connected via the prosthesis socket with the thigh, forms the counterpart. Ball head and socket insert thus form the so-called sliding pair and rub against each other when moving.
Cup insert and ball head are available in different materials. So can be selected in the cup inserts between ordinary polyethylene, highly crosslinked polyethylene or ceramic. The ball heads have a choice between metal and ceramic. In the sliding combination material combinations are possible.
Hip prostheses equipped with wear-resistant ceramics provide patients with high-quality care that allows them to regain a high level of quality of life over a long period of time. Ceramic has proven particularly useful in long-term use due to various advantages. Ceramic ball heads and cup inserts offer the best possible solution for active and younger patients as well as patients with metal allergy.
BIOLOX® high tech ceramic ball and socket inserts are available for most modular hip systems.
Actual Studies
Endoprosthetics: between aspiration and reality
Pain-free walking after hip joint replacement is no longer enough for most patients today, and many strive for extreme sports. But the load capacity and life of a hip prosthesis are - despite improvements - limits.
People's aspiration to stay mobile and fit for old age is increasing - even among patients with hip artificial joint replacement. Whether new material combinations, anchoring technology and the surgeons' know-how can meet these increased demands for longevity was the subject of a press conference of the German Society for Endoprosthetics in Frankfurt / Main. "About 95 percent of our patients are satisfied with their implants. We are challenged with the five percent with complications, "said Prof. Dr. med. med. Carsten Perka, Charité University Medicine, Berlin.
This does not only apply to patients who want to resume their normal running, swimming or cycling. "Rather, we are worried about the increased demands of patients who want to run marathons, practice yoga, do rock climbing and play football.
Such expectations are not impossible thanks to biomechanical findings, says Perka. "The ability to anchor, the sliding partners used, and the ability to model the 'normal' motion patterns of a hip joint have found their way into the latest generation of implants." However, the patient also needs to understand where the limits of an artificial hip joint are in terms of stress and longevity , Patient education in advance, which cleaned up with exaggerated expectations and illusions, was therefore necessary. Because: "An endoprosthesis, which lasts a lifetime, will not exist."
Two sliding pairs
That the life of an artificial joint depends not only on the choice of material, but also crucially on the skill of the surgeon, stressed. habil. Michael M. Morlock, Director of the Institute of Biomechanics at the Technical University of Hamburg-Harburg. Problems with implants that required revision were more likely to be due to the surgeon's approach and patient's behavior than to the design or material of established prostheses. Problems often occur at the interface with bone or other implant components, Morlock says.
For a few years, two pairs of sliding bearings have been established as standard: Ceramic head plus ceramic shell and the plastic shell with ceramic or metal head. These pairings guaranteed a correspondingly large mobility of the artificial joint. According to Morlock, the cement-free installation of the joint, which offers advantages for young patients, has also become established. Titanium is mainly suitable for the shaft and not for sliding mating. A ceramic head was less susceptible to corrosion than metal heads, which needed to be put on very carefully. Polyethylene is decreasing as a material for joint replacement.
The robot-based approach is currently being used reluctantly because a robot can only work rigidly in precisely defined milling paths. "But because the bone is a moving material, a rigid milling path is inappropriate," Morlock explained. In a separate study of 60 patients who received classic or robot-supported hip implants, the latter would have hobbled after the procedure, because the robot has also milled muscles.
Morlock, however, was convinced that robot-assisted surgery would enter a new era in five to ten years.
The expert emphasized the importance of movement for an hip endoprosthesis on the one hand, but also warned against exaggeration: "Moderate movement promotes, too much harm", so his motto. Complications would be due to premature wear on the metal parts, as by ion-particle release, the corrosion is promoted.
Morlock pointed out another problem: Due to the high expectations and price pressure for implants, new products would be launched on the market, even though there was no long-term clinical experience. Over the last decade, this approach would have resulted in an increased incidence of complications (implant fracture, dislocation, infections), revisions, and global compensation of over five billion euros in a handful of novel designs.
Morlock therefore advocated "establishing approaches that will allow new types of products to be safely launched onto the market in the future, to enable innovation in the first place." Results from other countries showed that further improvements in the longevity of artificial joints are not primarily due to Product innovation, but by addressing three factors, namely:
- obust implant systems that can be successfully used by all surgeons
- an improved, standardized and tested education and training as well as
- a realistic patient expectation that accommodates the inherent limitations of artificial joints


































 Loading ...
Loading ...


